
**By Steph Swarts, RMT, CNP** *Registered Massage Therapist | Certified Naturopathy Practitioner* 📅 Last Updated: January 17, 2026 ✅ Evidence-based recommendations from a licensed healthcare professional
As a Registered Massage Therapist and certified naturopathy practitioner, I see complaints about pain in the knee regularly in my practice. It’s one of the most common issues people face, and understanding what’s happening in that joint is the first step toward finding relief and preventing further problems.
Understanding Knee Anatomy and How Pain Develops
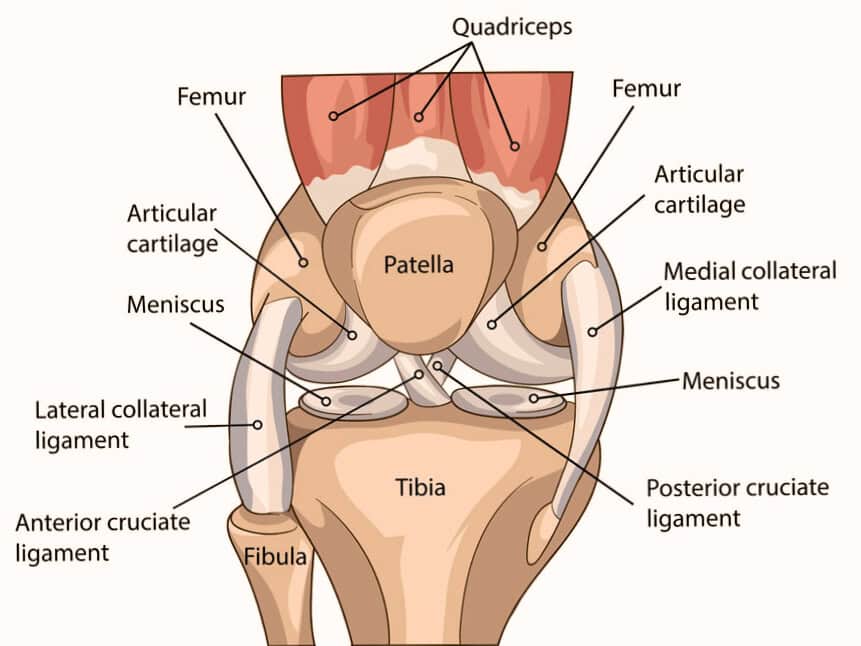
Your knee is a hinge joint bearing your entire body weight with every step. It consists of three bones – the femur (thigh bone), tibia (shin bone), and patella (kneecap) – held together by ligaments, moved by tendons, and cushioned by cartilage and menisci.
Pain develops when something in this system breaks down. Cartilage wears away, ligaments stretch or tear, tendons become inflamed, and menisci tear from injury or degeneration. Acute injuries happen suddenly from falls or sports, while chronic conditions develop gradually through inflammation and wear.
Most Common Causes of Pain in the Knee
Osteoarthritis is statistically the most common cause of knee pain, particularly in adults over 50. Research shows osteoarthritis accounts for nearly 80% of the global burden of arthritis and affects approximately 19% of American adults aged 45 and older. This degenerative disease occurs when cartilage wears away and bones rub together, causing progressive pain and stiffness.
Ligament injuries (ACL, MCL, LCL, PCL) commonly occur during sports or accidents. Meniscus tears happen from acute trauma or gradual degeneration. Tendinitis conditions like patellar tendinitis result from overuse. Bursitis occurs when fluid-filled sacs become inflamed. Patellofemoral pain syndrome causes pain that worsens with stairs and sitting. Baker’s cyst creates swelling behind the knee.
Understanding Pain by Location
The location of pain in the knee provides important diagnostic clues about the underlying problem:
Medial Knee Pain (Inner Knee)
MCL Injury: The most commonly injured knee ligament. Occurs from direct blows to the outer knee or twisting. Causes pain, swelling, and instability on the inner knee.
Medial Meniscus Tear: Pain along the inner joint line with catching, locking, and clicking. Worsens with twisting or squatting.
Pes Anserine Bursitis: Pain 2-3 inches below the inner joint line. Common in middle-aged women, runners, and people with osteoarthritis. Worsens with stairs and standing from chairs.
Medial Plica Syndrome: Irritated tissue fold causes clicking and pain when active after sitting.
Lateral Knee Pain (Outer Knee)
IT Band Syndrome: Most common cause of outer knee pain in runners and cyclists. The iliotibial band becomes tight and inflamed from repetitive friction. Creates aching or burning pain that worsens during activity. Often caused by weak hip muscles, sudden mileage increases, or running on tilted surfaces.
LCL Injury: Less common than MCL injuries. Results from blows to the inner knee or sudden stops with twisting. Causes outer knee pain, instability, and sometimes foot numbness.
Lateral Meniscus Tear: Pain on outer joint line with clicking, popping, and locking sensations.
Posterior Knee Pain (Behind the Knee)
Baker’s Cyst: Fluid-filled sac behind the knee creating fullness and tightness. Walking compresses the cyst, causing discomfort. Often accompanies arthritis or meniscus tears.
Hamstring Tendinitis: Pain where hamstring tendons attach behind the knee. Worsens with walking, especially uphill or on stairs.
Gastrocnemius Strain: Calf muscle strain causes pain behind the knee during the push-off phase of walking.
PCL Injury: Causes pain behind the knee, especially when kneeling or walking downhill.
Symptoms and Risk Factors
Common symptoms include swelling, stiffness (especially morning stiffness with arthritis), clicking or grinding (crepitus), instability, and locking sensations. Pain location – medial, lateral, anterior, or posterior – helps identify the cause.
Risk factors include age (cartilage breaks down after 50), excess weight (every extra pound adds 4 pounds of pressure on knees), previous injuries, muscle weakness, poor biomechanics, high-impact sports, and occupations requiring repetitive kneeling or squatting.
When to See a Doctor
Seek immediate attention for severe pain preventing weight-bearing, obvious deformity, rapid swelling, inability to extend or flex the knee, fever, or swollen/tender calf (possible blood clot). See a doctor for instability, pain persisting beyond 2-3 weeks, or signs of infection (warmth, redness, fever).

Diagnosis and Treatment
Doctors assess range of motion, perform stability tests, and determine pain location. X-rays detect fractures and arthritis. MRI scans show soft tissue damage. Joint aspiration helps diagnose gout or infection.
At-Home Care for Pain in the Knee
RICE protocol (Rest, Ice, Compression, Elevation) for acute injuries. Ice 15-20 minutes several times daily. Heat therapy works well for chronic stiffness. *** ATTENTION: Never put heat on a redness and warm-to-touch injury as this may cause more inflammation. Acute injuries (first 1-3 days) are ideal for ice/cold packs ONLY.
Topical anti-inflammatory products like Medistick can provide soothing, targeted relief directly to the affected area, offering a convenient alternative for those who prefer not to take oral medications or want additional pain management support.
Low-impact activities like swimming, water aerobics, and cycling maintain fitness without aggravating pain. Proper footwear and weight management are crucial. Using assistive devices when needed prevents further injury.
Medical Treatments
Corticosteroid injections provide weeks to months of relief, and are limited to 3-4 per year. Hyaluronic acid injections may reduce osteoarthritis pain for several months. Physical therapy is often the most effective treatment, addressing pain, weakness, and balance simultaneously.
Knee bracing provides stability. Surgical options include arthroscopy, partial replacement, or total knee replacement for severe cases.
Physical Therapy and Exercise
Strengthening quadriceps, hamstrings, and glutes provides better joint support. Effective exercises include straight leg raises, heel slides, wall sits, clamshells, and bridges. Stretching tight muscles (hip flexors, quadriceps, IT band, hamstrings, calves) is essential – hold 30 seconds, repeat 2-3 times.
Balance training reduces fall risk and strengthens stabilizing muscles. Foam rolling reduces muscle tension. Speak to a health professional to know when the right time is to add in strengthening exercises. If exercises cause your condition to get worse, stop immediately and let your health professional know.
Special Considerations for Cyclists
Proper bike setup prevents knee pain. Seat height is critical – at the bottom of the pedal stroke, knees should have 25-30 degrees of bend. When the pedal is at 3 o’clock, knees should be directly over the pedal axle. Use higher cadence (80-90 RPM) with lower resistance rather than grinding in high gears. Strengthen quadriceps (especially VMO), hips, and hamstrings. Stretch hip flexors, IT band, and calves daily. Professional bike fitting prevents cumulative damage.

Pain in the Knee Prevention Strategies
To prevent pain in the knee, aim to maintain a healthy weight. Also, build strong leg muscles through strength training. Then be sure to always warm up properly before activity and cool down afterwards. For older adults, warming up is even more critical because joints and muscles are stiffer. A 5-10 minute warm-up increases blood flow and prepares tissues for activity. After exercise, cool down with 5-10 minutes of light activity and gentle stretching to gradually lower your heart rate and prevent muscle stiffness.
Use correct form. Increase activity gradually (10% rule). Wear appropriate footwear and consider replacing worn shoes every 300-500 miles. Cross-train, varying your exercise activities rather than doing the same movement repeatedly, to avoid overuse. Listen to your body and rest when needed. Try incorporating tools in your post-workout stretch routine such as foam rolling or resistance bands to assist better recovery.
For IT band syndrome prevention specifically: strengthen hip abductors, stretch regularly, foam roll, vary running surfaces, and address bike fit issues.
Why cool-down is important for knee health:
- Helps remove lactic acid buildup that can contribute to muscle tightness
- Gradually returns heart rate and blood pressure to normal
- Allows muscles to release tension while still warm, making them more pliable for stretching
- Reduces post-exercise stiffness that can alter gait and put stress on knees
- Prevents blood pooling in the legs

Quick Comparison: Types of Pain in the Knee
Scroll horizontally to view full table on mobile →
| Condition | Pain Location | Common Causes | Typical Symptoms | Best Initial Treatment |
|---|---|---|---|---|
| Osteoarthritis | Deep in joint, all sides | Age, wear and tear | Morning stiffness, grinding, worsens with walking | Weight management, PT, ice/heat |
| IT Band Syndrome | Lateral (outer) side | Overuse, tightness, weak hips | Aching/burning on outside, worsens during walking/running | Rest, foam rolling, hip strengthening |
| MCL Sprain | Medial (inner) side | Direct blow, twisting | Pain on inner knee, instability | RICE, bracing, PT |
| LCL Sprain | Lateral (outer) side | Blow to inner knee, twisting | Outer knee pain, instability, foot numbness | RICE, bracing, PT |
| Baker’s Cyst | Posterior (back of knee) | Arthritis, meniscus damage | Swelling, tightness, fullness; worsens with walking | Treat underlying cause, ice, compression |
| Pes Anserine Bursitis | Medial, 2-3″ below joint line | Overuse, arthritis, obesity | Pain below inner knee, worse with stairs/walking | Rest, ice, hamstring stretching, topical relief |
| Meniscus Tear | Medial or lateral joint line | Twisting injury, degeneration | Locking, catching, clicking; can worsen with walking | RICE, physical therapy |
| Hamstring Strain/Tendinitis | Posterior (back of knee) | Sprinting, sudden acceleration | Sharp pain behind knee, worse with walking (esp. uphill) | RICE, gentle stretching, PT |
| Patellar Tendinitis | Front, below kneecap | Jumping, overuse | Pain below kneecap with jumping, stairs, walking | Rest, ice, eccentric exercises |
| ACL Tear | Deep in joint, center | Sudden stop, pivot, direct impact | Pop sound, rapid swelling, instability | RICE, bracing, possible surgery |
| PCL Injury | Posterior (back of knee) | Dashboard injury, fall on bent knee | Pain behind knee, worse with kneeling, walking downhill | RICE, PT, bracing |
| Patellofemoral Pain Syndrome | Front, around/behind kneecap | Overuse, muscle imbalance, poor tracking | Pain with stairs, squatting, sitting, prolonged walking | Quad strengthening, PT, activity modification |
| Medial Plica Syndrome | Medial (inner) side | Overuse, repetitive knee flexion | Clicking, pain after sitting, catching | Rest, stretching, ice |
| Gastrocnemius Strain | Posterior (back of knee/calf) | Sudden acceleration, tennis, basketball | Pain behind knee/calf, worse during push-off when walking | RICE, calf stretching, PT |
Frequently Asked Questions About Pain in the Knee
1. How do I know if my pain in the knee is serious or just temporary?
Temporary pain in the knee typically improves with rest within a few days. You can also try using ice, an anti-inflammatory such as Medistick, and elevating the knee to help speed recovery. Seek medical attention if you experience severe pain, significant rapid swelling, inability to bear weight, visible deformity, fever, or pain persisting beyond 2-3 weeks. Seniors should also see a doctor for instability or buckling due to fall risk.
2. Can I exercise with knee pain, or should I rest completely?
It depends on the cause. Complete rest can weaken muscles, especially in older adults. Low-impact exercises like swimming, water aerobics, cycling, or gentle walking are usually safe. Avoid activities that significantly increase pain in the knee. A physical therapist can help determine appropriate exercises for your condition.
3. Will losing weight really help my pain in the knee?
Yes, if weight is the issue, losing it will substantially help your knee pain. Every pound of body weight creates approximately 4 pounds of pressure on knees during walking. Losing just 10 pounds reduces knee stress by about 40 pounds per step. Many people with osteoarthritis experience significant improvement with modest weight loss.
4. Are knee injections worth it for managing chronic pain in the knee?
Results vary by individual and injection type. Corticosteroid injections provide temporary relief lasting weeks to months for inflammation. Hyaluronic acid injections may last several months and are specifically approved for knee osteoarthritis. PRP therapy shows promise for tendon and ligament issues. Discuss realistic expectations, potential benefits, and risks with your healthcare provider.
5. Can knee pain be prevented, or is it inevitable with age?
While some age-related changes are normal, significant knee pain is not inevitable. Many knee problems are preventable or can be delayed substantially. Maintaining healthy weight, building strong leg muscles, using proper form during activities, wearing supportive footwear, gradually increasing exercise intensity, and cross-training all reduce risk. Early intervention when problems first appear prevents progression to more serious conditions.
6. What’s the difference between medial, lateral, and posterior knee pain?
Medial pain (inner knee) often indicates MCL injuries, medial meniscus tears, pes anserine bursitis, or arthritis. Lateral pain (outer knee) commonly stems from IT band syndrome, LCL issues, or lateral meniscus problems. Posterior pain (back of knee) might indicate Baker’s cyst, hamstring tendinitis, or PCL injury. Pain location provides important diagnostic clues.
Final Thoughts
Managing knee pain successfully requires understanding your specific condition and implementing an appropriate treatment plan. Whether you’re dealing with medial, lateral, or posterior knee pain, early intervention and consistent management prevent minor problems from becoming major limitations.
From my perspective as an RMT and naturopathy practitioner, maintaining knee health is absolutely possible at any age. The key is staying active in appropriate ways, managing weight, building strength, and addressing problems early rather than waiting until function is severely compromised. With proper care, most people can maintain excellent knee function and continue enjoying their favourite activities for years to come.
About the Author

Steph Swarts, RMT, CNP
Steph Swarts is a registered massage therapist and certified naturopathy practitioner with 17+ years of clinical experience helping clients optimize their health through evidence-based supplementation and holistic wellness strategies.
Professional Credentials:
- Registered Massage Therapist (RMT) – Licensed in Ontario, Canada
- Certified Naturopathic Practitioner (CNP)
- Raindrop Technique Practitioner (RTP)
- 17+ years in clinical practice
- Specialized training in Prenatal Massage Therapy
Clinical Expertise:
“As a healthcare professional with naturopathic training, I evaluate supplements using the same rigorous standards I apply in client care. My recommendations prioritize:
✅ Safety: Thorough evaluation of quality and purity
✅ Evidence: Backed by peer-reviewed research
✅ Clinical relevance: Real-world effectiveness for performance and recovery
✅ Professional standards: Third-party testing and manufacturing quality
Over 17+ years, I’ve guided hundreds of clients through their health journey, injury recovery, and overall wellness. Every recommendation reflects my professional commitment to evidence-based natural health.
Professional Memberships:
- Registered Massage Therapist with CMTO
- Member of RMTAO
- Certified Naturopathy Practitioner with NCCAP, CPD, and CMA
- Raindrop Technique Practitioner with Institute Of Energy Wellness Studies
📧 Contact: [email protected]
🌐 Website: www.stephswarts.com
📱 Social: https://www.facebook.com/StephanieJSwarts
Professional Disclaimer: Information provided is for educational purposes based on clinical expertise and current research. This does not replace individualized medical advice. Consult your healthcare provider before starting any supplement regimen, especially if you have pre-existing conditions or take medications.
Here’s a properly formatted references section you can add to the end of your article:
⚠️ Affiliate Disclosure: This article contains affiliate links to products I recommend, including from Amazon. If you purchase through these links, I may earn a small commission at no additional cost to you. As a registered massage therapist with 17+ years of experience, I only recommend products I personally use or genuinely believe will benefit your health and wellness. All opinions and recommendations are based on my professional expertise and clinical experience.
References
- Cleveland Clinic. (2024, October 7). Knee Osteoarthritis: Symptoms, Stages, Causes & Treatment. Retrieved from https://my.clevelandclinic.org/health/diseases/21750-osteoarthritis-knee
- Nguyen, U. S., Zhang, Y., Zhu, Y., Niu, J., Zhang, B., & Felson, D. T. (2011). Increasing Prevalence of Knee Pain and Symptomatic Knee Osteoarthritis. Annals of Internal Medicine, 155(11), 725-732. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC3408027/
- World Health Organization. (2023, July 14). Osteoarthritis. WHO Fact Sheet. Retrieved from https://www.who.int/news-room/fact-sheets/detail/osteoarthritis
- Cui, A., Li, H., Wang, D., Zhong, J., Chen, Y., & Lu, H. (2020). Global, regional prevalence, incidence and risk factors of knee osteoarthritis. EClinicalMedicine, 29-30, 100587. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC7704420/
- Cleveland Clinic. (2025, September 25). Pes Anserine Bursitis: What It Is, Symptoms & Treatment. Retrieved from https://my.clevelandclinic.org/health/diseases/pes-anserine-bursitis
- Cleveland Clinic. (2021, October 28). Iliotibial Band Syndrome (ITBS): Causes, Symptoms & Treatment. Retrieved from https://my.clevelandclinic.org/health/diseases/21967-iliotibial-band-syndrome
- American Academy of Family Physicians. (2005, April 15). Iliotibial Band Syndrome: A Common Source of Knee Pain. Retrieved from https://www.aafp.org/pubs/afp/issues/2005/0415/p1545.html
- Johns Hopkins Medicine. (2024, May 1). Iliotibial Band Syndrome. Retrieved from https://www.hopkinsmedicine.org/health/conditions-and-diseases/iliotibial-band-syndrome





